
Case Report | DOI: https://doi.org/10.31579/2578-8868/170
1Functional Surgery Working Group, Department of Neurosurgery of the Institute of Neurology and Neurosurgery, Havana, Cuba.
2Endoscopic and Skull Base Surgery Working Group, Department of Neurosurgery of the Institute of Neurology and Neurosurgery, Havana, Cuba.
3Spinal Surgery Working Group, Department of Neurosurgery of the Institute of Neurology and Neurosurgery, Havana, Cuba.
4Department of Clinical Neurophysiology of the Institute of Neurology and Neurosurgery, Havana, Cuba.
*Corresponding Author: Duniel Abreu Casas, MD, Institute of Neurology and Neurosurgery of Cuba, Department of Neurosurgery, Spinal Surgery Working Group, 29th street to D, Vedado, Habana. Cuba.
Citation: Duniel Abreu Casas., Orestes Lopez Piloto., Norbery J. Rodríguez de la Paz., Oscar Quiroz Osorio., Emmanuel Batista Geraldino., et al., (2021) Selective Neurectomy of the Vestibular nerve through a Retrosigmoid approach for the Treatment of vertigo in Ménière's Disease. J. Neuroscience and Neurological Surgery. 8(4); DOI:10.31579/2578-8868/170
Copyright: © 2021 Duniel Abreu Casas, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 13 March 2021 | Accepted: 26 April 2021 | Published: 05 May 2021
Keywords: ménière's disease; retrosigmoid approach; treatment
Ménière's disease (also known as Ménière's vertigo) is a condition characterized by disabling recurrent vertigo, sensorineural hearing loss, otic fullness, and tinnitus. There are various treatments to manage this entity, however, in certain cases, the lack of improvement with less aggressive strategies and the great impact on the quality of life of the patient requires radical procedures such as vestibular neurectomy. By means of a lateral suboccipital approach (retrosigmoid craniectomy) the best exposure of the vestibular nerve, its selective isolation and section is obtained, also allowing to preserve hearing and the entire facial nerve supported with neurophysiological monitoring techniques.
Ménière's disease is a complex and multifactorial disease of the inner ear, characterized by a combination of episodic vertigo with neurovegetative symptoms, sensorineural hearing loss, auditory fullness and tinnitus. Different hypotheses on the mechanism of the disease have been proposed. But currently there is no universally accepted theory about the underlying pathophysiology. Controversy about the relationship between endolymphatic hydrops and Ménière's disease has always been existing, although the cause remains unclear [1].
In its most severe forms it is a very disabling disease1, mainly due to the vertiginous picture, preventing the patient from leading a normal life. When the disease is resistant to conservative treatment, a vestibular neurectomy should be considered [2,3].
Over the years, different neurosurgical or otoneurological approaches have been proposed to control seizures by sectioning the vestibular nerve and trying to preserve hearing while respecting the cochlear fibers or the structure of the inner ear. One of the treatment options is to perform a neurectomy through a retrosigmoid craniectomy [3,4]
It is a 37-year-old man, of skillful handcraft, with no other pathological antecedents, with disabling recurrent rotational vertiginous crises of 5 years of evolution, with severe worsening in recent months, and with a feeling of increasing and continuous instability, causing great impact on their quality of life. He also has severe hearing loss in the right ear. There is no improvement with vestibular rehabilitation exercises, or with the administration of other medical treatments. After the case was evaluated by the Neurosurgeons Collective in the Skull Base Pathology section of the Institute of Neurology and Neurosurgery of Havana, a selective neurectomy of the vestibular nerve is proposed through a right retrosigmoid approach.
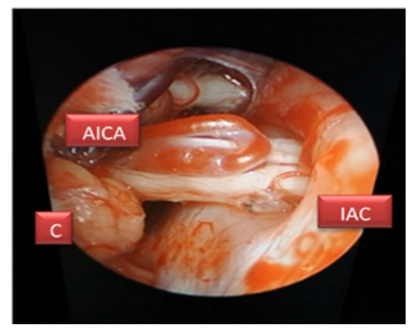
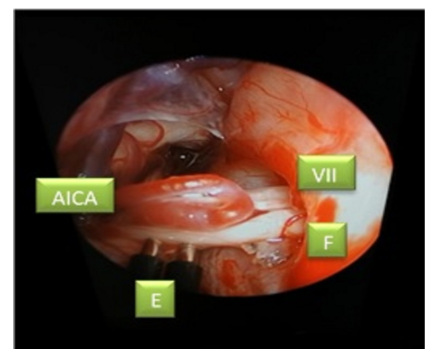
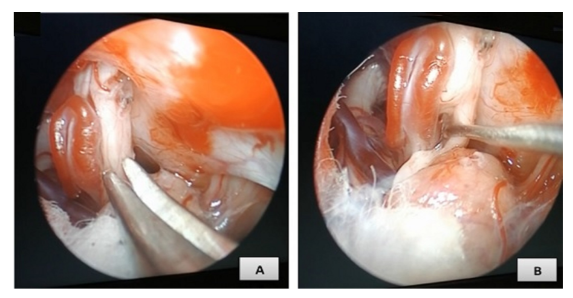
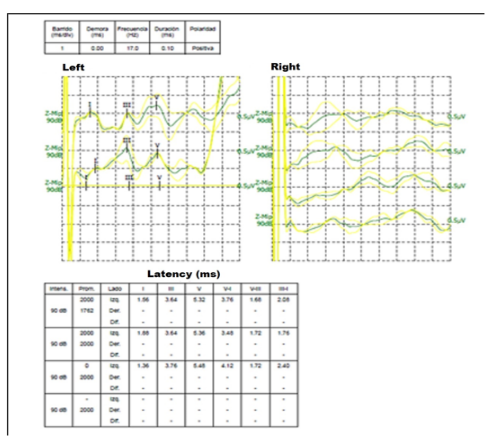
In the ¾ prone position, head in the Mayfield-kees head, lateralized to the left (Figure. 1), an approach was performed by means of a retrosigmoid craniectomy, about 2cm in diameter. After the dural opening and with the use of a 0 ° endoscope (Karl-zeiss), the cerebellum is carefully separated to reach the cerebellomedullary cistern, where cranial nerves IX, X and XI are identified, ascending later until locating the facial complex - vestibulocochlear at the level of the IAC (Figure. 2). After dissection of the arachnoid membranes that cover the vestibulocochlear nerve, identification of the Antero Inferior Cerebellar Artery (AICA) is performed, which is forming a loop over the vestibule-cochlear nerve, indentating the complex and partially separating it. The different nerves of the complex are identified below, according to existing references in the scientific literature. Neurophysiological monitoring was used at different intensities to identify the facial nerve and respect its anatomical integrity (Figure. 3). Subsequently, the vestibular nerve was dissected, selectively separating it from the cochlear nerve, and the neurectomy was performed respecting the fibers of the cochlear nerve to preserve the residual hearing of the patient (Figure. 4). A careful hermetic dural closure was performed with 4.0 braided suture, without the need for dural plasty. After surgery, the patient spent 24 hours in the Intensive Care Unit. In the control CT, no complications derived from the approach were observed, such as the existence of pneumocephalus or cerebellar contusions due to retraction (Figure. 5). He was discharged 4 days after surgery,

In subsequent clinical follow-up studies, the patient has experienced a great improvement, with remission of the vertiginous crises. Hearing has experienced a decrease in its level without recovery, after 6 months of control. Finally, it should be noted that given the severe previous right hearing loss and the great impact that Ménière's disease had on their quality of life, the patient and the family reported great satisfaction with the surgical result.

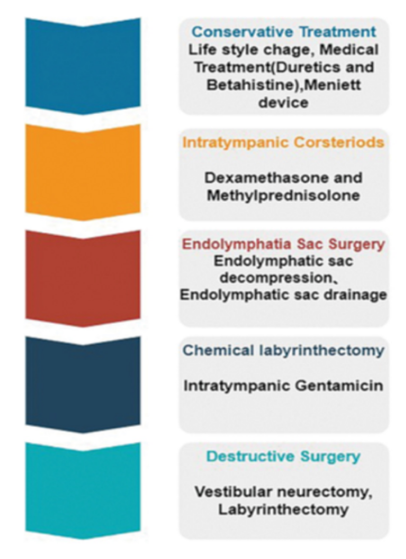
Ménière's disease was described by the French physician Prosper Ménière in 1861, going from being considered a mental illness to a clearly defined entity. Since then, multiple treatments have been proposed to improve the vertiginous crises that constitute the most disabling fact of the disease [5]. In a more conservative way, drug treatments such as loop diuretics (acetazolamide), betahistine, etc., are used to move to more aggressive therapies such as injections of gentamicin or intratympanic corticosteroids, achieving control of the disease between 72-95 %, although it can be associated with hearing loss in a significant percentage of cases [6,7].
It is considered that when this ablative therapy fails, there is the alternative of performing a surgical treatment for which destructive surgeries are performed that entail a complete loss of hearing (labyrinthectomies through its different routes) or performing a selective vestibular neurectomy, managing to respect the hearing [3,7]. There are different surgical routes for this purpose. Historically, in 1898 Krause performed the first neurectomy of the VIII cranial nerve through a retrosigmoid intracranial route. Subsequently, it would be Dandy, one of the pioneers of neurosurgery, who proposed a selective vestibular neurectomy, being performed by McKenzie for the first time in 1936, becoming the approach of choice for many years [6,7]. Later in 1961, House described an extradural microscopic approach to the internal auditory canal through the middle fossa to avoid the complications that occurred in intradural approaches. With this approach, only a neurectomy of the upper vestibular nerve was performed, with poor dizziness control rates. Fisch [9] and Glasscok modify House's technique to also perform a section of the inferior vestibular nerve, getting good control of seizures and respecting hearing. However, they presented high rates of facial paresis, which is why this approach was not widely used [10].
Currently, thanks to advances in microscopic, endoscopic and neuroanesthesia neurosurgery, the complications of posterior fossa approaches are minimal. By means of the retrosigmoid approach, the best exposure of the vestibular and cochlear nerve is achieved, being able to perform a complete vestibular neurectomy respecting the cochlear nerve, being equally easy to fully identify and respect the facial nerve with the help of intraoperative neurophysiology.
The vestibular nerve is anterior and superior to the cochlear nerve in its pre-canalicular segment. Also according to some authors, there are differences in the coloration of these, the vestibular nerve being more grayish. Likewise, a fine arteriole can often be identified that is located between the cleavage plane of both nerves, which can be a useful reference [3,4] although it is true that this separation can be difficult to objectify. It should be noted that there may be crossed vestibular fibers in the trunk of the cochlear nerve, for this reason it has been proposed to perform a small section of about 0.5 mm of the cochlear nerve in the area adjacent to the vestibular, to seek to perform a complete neurectomy, without worsening hearing [3].
The control rates using this approach are excellent, being 90-100%. There is a worsening in hearing in 20% of patients, although there are authors who report an improvement rate of 25%. The permanent facial paresis rate is non-existent in most series [3,4]. We believe that the use of neurophysiological monitoring is essential to respect the facial nerve and not generate significant morbidity. The complications derived from brain retraction, with careful microsurgical management, are also minimal. Usually achieving a hermetic dural closure can be difficult, so to prevent CSF fistula various materials such as dural plasties or bioglues can be used, with which this complication is reduced to a minimum, being around 10%,
The retrosigmoid approach allows an excellent exposure of the vestibular nerve, making it possible to perform a complete and selective neurectomy, with good clinical results.
The help of intraoperative neurophysiology is essential for the correct identification and differentiation of the facial nerve.
Microscopic and endoscopic management and microsurgical instruments are essential to avoid problems in cerebellar retraction, and allow it to be a well-tolerated approach with few complications.
Familiarization of the neurosurgeon with this procedure and joint management with otorhinolaryngology allow adequate control of the disease.
CONFLICT OF INTERESTS
The authors declare that they have no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
